(1).jpg)
Ophthalmic Imaging History
Early Retinal Imaging: The Beginnings of Ophthalmic Photography
Early retinal imaging -- The origins of (retinal) ophthalmic photography go back around 150 years when Drs Jackman and Webster, in the USA, published the first robust account of capturing images of the human retina.
Their two seminal papers from 1886 describe the process and results of the first successful retinal image from a living human. Paradoxically, whilst they managed to successfully record recognisable retinal images after (only) a two-and-a-half-minute exposure time, they could not afford the publication costs to reproduce the actual images in the journals of the time.
Their articles contained only line-drawing representations of their promising results, but they are generally considered to be the first such published ‘images’. As the reproduced linedrawings showed only the sketchiest outlines of the human optic disc, it was of no real use as a diagnostic investigation.
Development of Photography and Contributions of Other Pioneers
However, it was an important development, coming 50 years after the introduction of what we would now consider real ‘photography’ in 1839, when Louis Daguerre produced the first permanent image as his “Daguerreotype”.
.jpg)
Others may well have managed to successfully produce retinal images in living humans prior to Jackman and Webster, but theirs were the first to be published. Lucien Howe, “E. Barr of Buffalo” and “Elmer Starr of Buffalo” have all been mentioned as such early pioneers and, ironically, the latter two are one-in-the-same person, due to typographical errors at the time.
In 4 reality, Howe and “Starr/Barr” worked in the same department in Buffalo Eye and Ear Infirmary, so their results were all part of the same research effort, but their early work was trumped by Jackman and Webster’s articles.
The concept of ‘publish or perish’ has a very long history. Clearly, these early inventions were far from practical or affordable and were not diagnostic or (trans)portable. Very long exposures were required, even with exceptionally intense light sources.
These were not comfortable for the patient so, in effect, only already blind eyes could be normally imaged at the time. What was missing was a practical and affordable optical instrument and suitable light-source to move these inventions forwards.
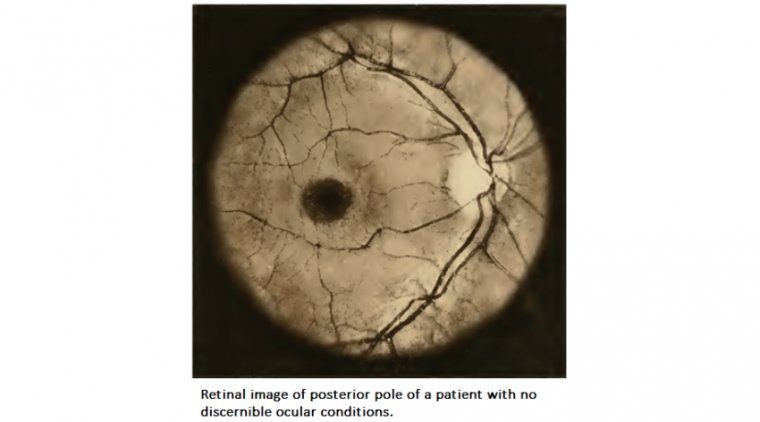
Essential inventions of optical instruments were soon to change all that. From 1899 Friedrich Dimmer of Vienna demonstrated truly wonderful (monochrome) images of the human retina after a close collaboration with Zeiss Jena, who developed a radical design of fundus camera.
.jpg)
The most profound element of their later design was that it utilised the Gullstrand principle of co-axial illumination coupled with viewing through the ‘anulus’ of the optics. This produced images free of the massive corneal reflex previously exhibited on all attempts at retinal imaging.
Those images are very impressive, even by modern standards and were the first diagnostically relevant retinal images. Sadly, their retinal camera design was a one-off as it was massively expensive to build and equally huge.
Decades on, Zeiss, of course, along with many other manufacturers, have refined their inventions to result in the small, portable, and affordable retinal imaging devices to which we now have access. From film to digital and all that stuff People may not be aware that colour photography has also got a very long history.
Eastman Kodak released the eponymous Kodachrome (transparency) film as far back as 1935. Polaroid instant-print colour film was released in 1963 and Kodak had already released high-speed monochrome Tri-X film back in 1954.
These advances in recording media, coupled with Harold Egerton’s invention of the first rechargeable electronic flash tube in 1931, set the scene for enabling modern ophthalmic imaging. It was only after another 30-40 years that digital retinal imaging became a practical reality.
The early systems for anterior and posterior segment imaging were commonly based on the Sony 3-chip still video from 1980 and after 1984, Canon’s first digital electronic still camera, largely replacing the workhorse Nikon F2 film camera backs and motor-drives.
The digital images were, in comparison to the high-definition colour systems in use today, rather crude. They did, however, give us access to ophthalmic images which could be easily shared, and indeed copied (with the associated problems that created).
We were amazed and enthused in equal measure. With the advent of expanding activities, including those to screen for conditions such as diabetic retinopathy and glaucoma, there was massive competition amongst manufacturers for affordable and indeed more portable devices to satisfy the tremendous need for higher quality retinal imaging.
It may surprise many to find out that the first mobile phone with an integral digital camera was released (by Kyocera Corporation) only in 1999. Just over twenty years on, we have in-phone digital imaging capabilities which far surpass anything we could have dreamt of for our hospital clinical imaging in the late 1980s.
There have been some successes in pairing mobile phone cameras to ophthalmic imaging devices, particularly when applied to rural screening activities. The advent of digital imaging, however, created its own problems.
No longer did we have to buy, expose, and then get films processed, mounted, sorted, labelled, and stored. Rather, we were suddenly faced with totally inadequate local IT and storage systems to cope with the demands of an ophthalmology department.
Problems were even more exaggerated with the introduction of optical coherence tomography (OCT) and, more recently, confocal scanning (laser) ophthalmoscope devices (cSLO) which together with other routine imaging techniques regularly produce gigabytes of data.
Move over radiology - the new ‘ophthalmology massstorage needs’ were taking over. Enough about the What, When and How, what about the Who? Over the years the practice of ophthalmic imaging (internal and external eye) was to change from being the remit only of interested and skilled clinicians (predominantly ophthalmologists of course) to become the major preserve of dedicated medical and ophthalmic imaging professionals.