
iHealthScreen has been granted a full US patent for its iPredict glaucoma detection model by the US ...
read more
ENTOD Pharmaceuticals, a Mumbai-based company, has achieved a significant milestone in eye care with...
read more
EyeSouth Partners, a prominent eye care-focused management services organization, announced its newe...
read more
In an inspiring leap towards health equity, a new eye health project in Malawi has successfully brou...
read more
Caplin Steriles Limited (Caplin), a subsidiary of Caplin Point Laboratories Limited, has received fi...
read more
Medevise Consulting, a strategic consultancy specializing in the ophthalmic sector, announced that i...
read more
Ocular Therapeutix announced a significant shift in its leadership structure, as Executive Chairman,...
read more
Kiora Pharmaceuticals announced that it has secured a grant from the Choroideremia Research Foundati...
read more
Oasis Medical has recently unveiled its latest product, the SOFT PLUG Extended Duration 180-T Tapere...
read more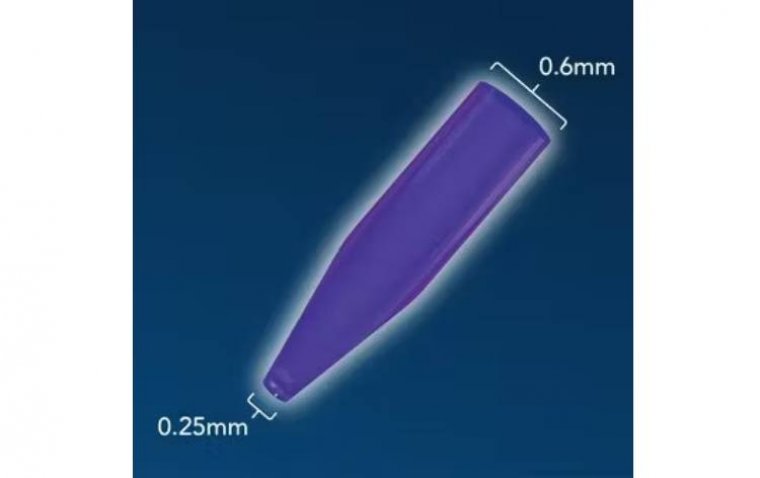
Ocugen has received approval from the FDA for an amendment to their investigational new drug (IND) a...
read more
 More
More
